Scientists at St. Jude Children’s Research Hospital and the University of California, San Francisco used a naturally occurring carbon isotope and exhaled CO2 to catch bacterial infections.MEMPHIS, Tenn., March 18, 2026 /PRNewswire/ — Bacterial infections can be difficult to distinguish from viral infections and noninfectious inflammation, but a simple breath test may change that. A study led by St. Jude Children’s Research Hospital and the University of California, San Francisco, shows how molecules that are only broken down by infecting bacteria, and not by gut bacteria, can be used to confirm infection. By enriching these molecules with a naturally occurring carbon isotope, the researchers found that carbon dioxide produced when they break down is easily detected in a breath test using inexpensive infrared scanners. This proof-of-concept study sets the stage for clinical testing and has the potential to offer essentially any health care space the ability to rapidly and affordably identify bacterial infection, or lack thereof, reducing unnecessary antibiotic prescriptions. The findings were published today in ACS Central Science.
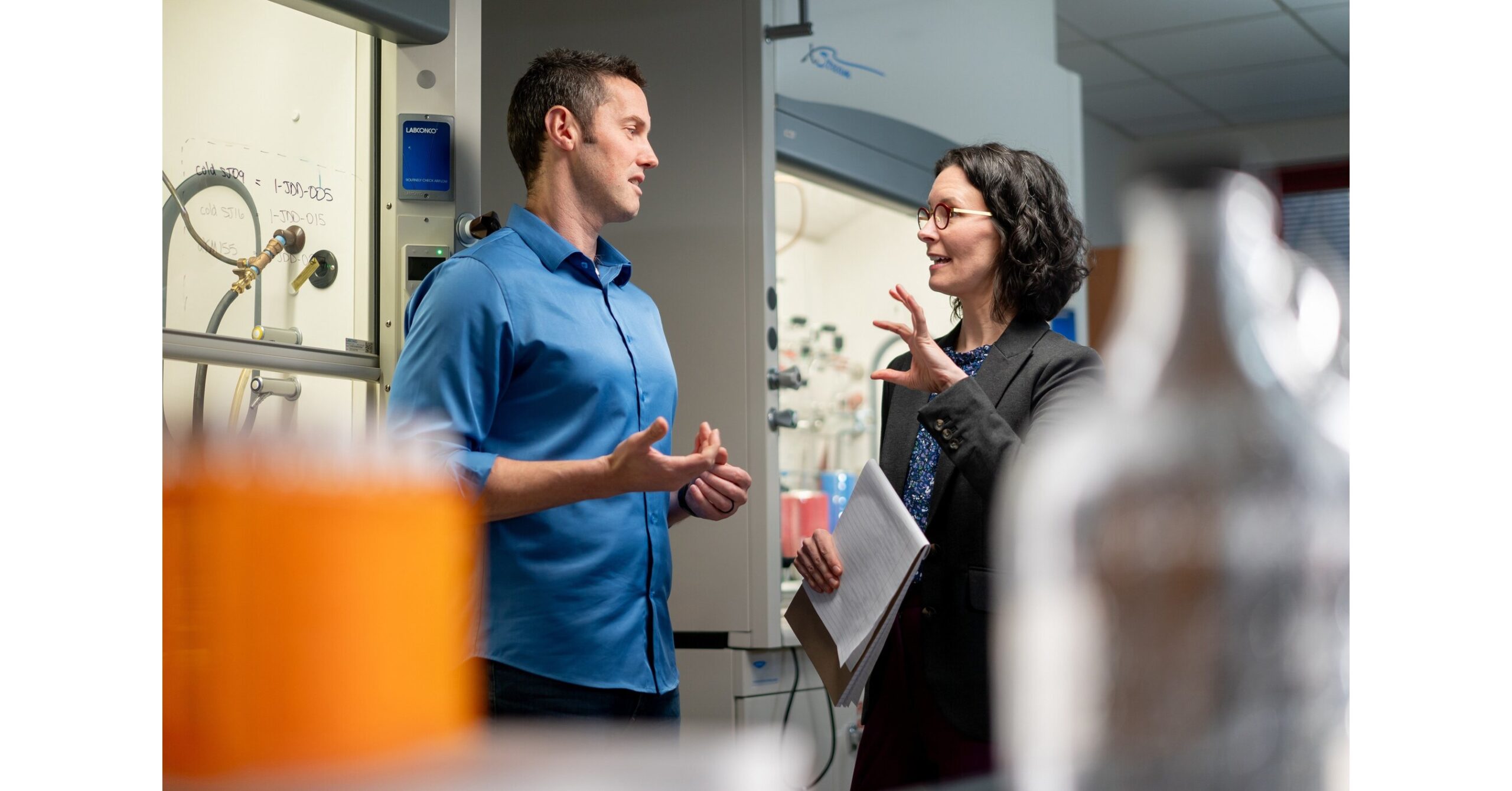
Published today in ACS Central Science, co-corresponding author Kiel Neumann, PhD, St. Jude Department of Radiology, and co-author Amanda Green, MD, St. Jude Department of Infectious Diseases, demonstrated how mannitol made with carbon-13 and a breath test can be used to immediately detect a bacterial infection.
Traditionally, bacterial infections are diagnosed by taking a sample and growing it in a laboratory culture. This process can take days. The breath test approach may offer a significantly more accessible rapid test.“When a patient presents with certain symptoms, doctors already have an idea of the likely pathogens,” co-corresponding author Kiel Neumann, PhD, St. Jude Department of Radiology, says. “We hope that this test could be a quick screening tool to know whether it’s a bacterial infection or not.”Infrared detection for bacterial infectionIn a recent trial to detect bacterial infection using positron emission tomography (PET) scans, Neumann noticed that a radiolabeled form of mannitol — a molecule metabolized only by bacteria — was not absorbed by the body’s natural gut microbes. Building on this, the researchers created a version of mannitol enriched with the naturally occurring isotope, carbon-13 instead of the stable isotope, carbon-12. When administered intravenously, this carbon-13 molecule is broken down for nutrients only by infecting bacteria, producing a labeled carbon dioxide byproduct, which is then exhaled. That exhaled carbon dioxide can be measured using an inexpensive nondispersive infrared (NDIR) spectroscopy tabletop instrument, and could successfully detect signs of myositis, bacteremia, pneumonia and osteomyelitis.The researchers focused on pathogens common in clinical settings, including Staphylococcus aureus, Streptococcus pneumoniae and Escherichia coli, but also included Salmonella enterica. This pathogen is not usually a concern for healthy immune systems but poses significant problems in people who are immunocompromised, such as those with sickle cell disease, where infection and inflammation are very often conflated.“A patient might complain of nonspecific symptoms, like pain and swelling, but it is likely a vaso‑occlusive crisis — purely inflammatory,” Neumann says. “It could be an infection, however, and because the risk of missing an infection is high, they get antibiotics anyway, even if unnecessary.”The study represents the first step toward a safe, straightforward and easily obtainable test for bacterial infection and sets the stage for future clinical studies to explore the widespread feasibility of the test. “We want to explore how we can use this technology to have an impact at ground level — patients checking into urgent care or an emergency room, for example,” Neumann says. “There’s a lot of work to do in humans to establish a true protocol, but we are very enthusiastic about its potential.”Authors and fundingThe study’s co-corresponding author is David Wilson, University of California, San Francisco. The study’s first author is Marina López-Álvarez, University of California, San Francisco. The study’s other authors are Sang Hee Lee, Anju Wadhwa, Mohammad Yaqoob Bhat, Jung Min Kim, Anil Bidhar, Joseph Blecha, Robert Flavell, Renuka Sriram and Joanne Engel, University of California, San Francisco; Shari Dhaene and Tom Desmet, Ghent University; Marshall McCue, Sable Systems International; Michael Ohliger, University of California, San Francisco and Zuckerberg San Francisco General Hospital; and Tyler Simmons, Spenser Simpson, Jeffrey Steinberg, Amanda Green and Jason Rosch, St. Jude.The study was supported by the National Institutes of Health (R01-EB030897, R01-AI181378, R01-AI161027, R21-AI164684, R01-EB028338 and R01-AI192221), the Cystic Fibrosis Foundation (20A0) and the American Lebanese Syrian Associated Charities (ALSAC), the fundraising and awareness organization of St. Jude.St. Jude Children’s Research HospitalSt. Jude Children’s Research Hospital is leading the way the world understands, treats, and cures childhood catastrophic diseases. From cancer to life-threatening blood disorders, neurological conditions, and infectious diseases, St. Jude is dedicated to advancing cures and means of prevention through groundbreaking research and compassionate care. Through global collaborations and innovative science, St. Jude is working to ensure that every child, everywhere, has the best chance at a healthy future. To learn more, visit stjude.org, read St. JudeProgress,a digital magazine, and follow St. Jude on social media at @stjuderesearch.SOURCE St. Jude Children’s Research Hospital









Leave a Reply